|
Role of Biotin and its effects
on health
Professor Toshiaki Watanabe
School of Humanities for Environmental Policy and Technology
Himeji Institute of Technology
|
 |
Introduction
Biotin is contained in various food products, but little is known
about it. Recently, biotin has been found to be greatly involved
in our health. In this report, we will discuss the role of biotin
in a living body, particularly, the involvement of biotin in dermatopathies,
such as atopic dermatitis, which is attracting great attention in
recent years. Furthermore, since biotin will soon be approved as
a food additive, we will introduce the importance of biotin as a
dietary supplement.
|
1. What's Biotin?
Biotin is a water-soluble vitamin found in a wide range of food such
as liver, yolk and cereals. It is also synthesized by enteric bacteria.
Therefore, except for people with extremely unbalanced diet or intestinal
disorders, generally, biotin deficiency is rarely found among people
with ordinary diet. Biotin deficiency is possibly caused by reduction
of biotin intake, inhibition of biotin absorption, inborn errors of
metabolism, etc. In our bodies, biotin acts as a coenzyme, supporting
the function of carboxylase. Since carboxylase is an enzyme involved
in glyconeogenesis, fatty acid synthesis, amino acid metabolism, etc.,
biotin deficiency disturbs the energy metabolism as well as various
physiological functions. Deficiency of biotin also results in immune
depression and reduced collagen synthesis. As a result, biotin deficiency
is known to induce dermatological symptoms such as seborrheic eczema
and psilosis, opportunistic infection and neuritis in human, although
its direct involvement is still unclear. A recent report has suggested
that biotin levels decrease along with the gestational stage in pregnant
women. In an animal experiment, biotin deficiency in the mother induced
fetal anomaly.
Biotinidase is an enzyme involved in biotin metabolism, which liberates
biotins bound to proteins within the digestive tract. As a carrier
protein, it is also involved in biotin absorption and transport. Therefore,
symptoms of biotin deficiency are also observed in cases of carboxylase-
or biotinidase-related impairment. "Egg white injury", found
in those consuming a large amount of raw egg over a long period of
time, is also caused by biotin deficiency.
Consequently, biotin has been otherwise known as "vitamin H"
in which "H" stands for "Haut", the German word
for "skin". Since the old days, biotin has been known as
a vitamin closely related to the skin. Therefore, biotin has been
used as a remedy for dermatoses, but rarely after the recent development
of new drugs. Chinese medicine formulations used for dermatoses also
contain
a large amount of free biotin.
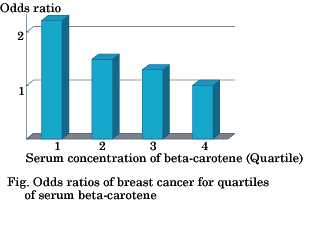
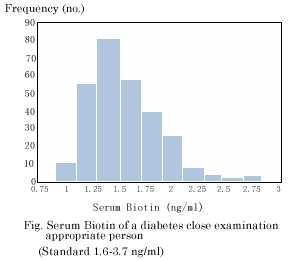
2. Diabetes and Biotin
Palmoplantar pustulosis and palmoplantar pustular osteoarthropathy
are diseases in which many rashes and pustules appear on the palms
and soles. To date, there is no definitive treatment for such diseases.
The blood biotin levels in these patients are less than half of
the normal level, and about 60% of the patients have diabetes as
complications. Oral administrations of a large dose (9 mg/day) of
biotin to the patients not only eliminated the rashes and bone aches
but also reduced their blood glucose levels, indicating the efficacy
of biotin dosing against diabetes. When biotin was continuously
administered in combination with an antidiarrheal to insulin-independent
diabetes patients, the blood glucose levels were actually decreased
to a normal range in all of the patients tested. Even in insulin-dependent
diabetes patients, biotin dosing resulted in normal blood glucose
levels. The mechanism of biotin's action is still unclear, but since
biotin is involved in sugar metabolism, it is suggested that biotin
administration has promoted sugar metabolism, which lead to reduction
in the blood glucose levels.
3.Infant and Biotin
Infants having milk allergy or inborn error of metabolism are fed
with special therapeutic milk preparations. In our country, biotin
cannot be added to food products, because it has not been approved
as a food additive.
Therefore, biotin is not added to the milk powders or special therapeutic
milk preparations that are currently in use. Especially, therapeutic
special milk preparations are prepared using purified raw materials,
so some products barely contain biotin. The average biotin content
in the commercially available powdered milk and special therapeutic
milk preparations are 1.04 and 0.45 μg/100 kcal, respectively, which
are extremely low compared to the level (1.5μg/100 kcal) recommended
by FAO/WHO (United Nations Food and Agriculture Organization). Therefore,
insufficient biotin intake is greatly concerned for artificially
fed infants who are fed with such powdered milk in our country.
Recently, it has been reported that serum biotin levels in atopic
dermatitis patients are less than half of the normal level. Moreover,
when infants diagnosed as milk allergy were fed with special therapeutic
milk preparations, diaper rash-like rashes and erythema around the
eyes and mouths appeared. The erythema disappeared when biotin was
administered to such infants. These reports indicate that biotin
is involved in the development of atopic dermatitis. The biotin
content in baby food is within the range of 0−58.5μg/100g. In general,
biotin content is higher in cereal- or meet-based food but lower
in juice beverages and refreshments based on dairy products. Some
products contain no biotin at all.
In general, infant meals have poor variety, and powdered milk has
low biotin content. In addition, functions of digestive tracts are
immature in infants, allowing little production and absorption of
biotin. Therefore, the risk of biotin deficiency is higher in infants.
Biotin deficiency hinders skin formation, resulting in a state susceptible
to external stimuli. Therefore, a great attention must be paid to
the biotin intake in infants.
4.Bitoin dysbolism
In some patients who have been diagnosed as atopic dermatitis, remission
cannot be observed for more than 5 years. Among such patients, 3−4%
are found to have low biotinidase activities. In addition to the
reduced enzyme activity, the biotin levels in such patients are
less than 10% of those of healthy subjects. Biotin administration
(5 mg/day) resulted in the elimination of the eczema formed on their
faces, indicating that some of the intractable cases of atopic dermatitis
are caused by deficiencies of biotin-related enzymes such as biotinidase
and carboxylase.
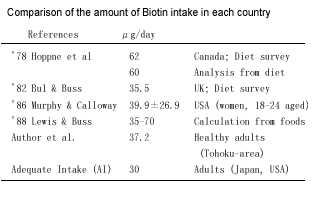
5. Biotin as supplement
In the United States and European countries, biotin is used in daily
food and vitamin tablets, and its importance is widely accepted.
Meanwhile, in our country, biotin is not used as a dietary supplement,
since it is not approved as a food additive. The reason for its
disapproval is not because biotin has any toxicity, but because
its nutritional importance has not been sufficiently acknowledged.
This is obvious from the fact that biotin is approved as a remedy
for dermatoses.
The recommended dietary allowance for biotin has been first established
in the sixth revision of nutritional requirements for the Japanese.
The recommended dietary allowance for biotin is 30μg/day for adults.
The maximum acceptable intake has not been established, since an
excessive dosing (10−100 mg) of biotin showed no side effects, although
it has not been tested in healthy subjects. Nevertheless, biotin
was not included in the fifth revision of Standard tables of food
consumption in Japan, although folic acid and vitamin B12 were newly
included. In our country, health-promoting food has been formulated
in April 2001, which has clearly determined the specified health
food and the food with nutrient function claims. For the food with
nutrient function claims, labeling standards and specifications
have been established for 12 vitamins including biotin and 2 minerals.
According to the ingredient specification for biotin, the maximum
and minimum allowable dosages are 500μg and 10μg, respectively.
Moreover, the nutrient function claim approved for biotin is "biotin
is a nutrient which supports the health maintenance of the skin
and the mucous membrane". As mentioned above, biotin is greatly
involved in the health of our skin, so biotin supplement should
have a great value.
6. Conclusion
It is generally considered that biotin deficiency does not exist,
but the possibility of latent or non-manifest biotin deficiency
still remains. Moreover, it has been suggested that biotin deficiency
can worsen the intractable cases of atopic dermatitis or diabetes.
Nevertheless, the physiological function of biotin has not been
sufficiently understood, requiring further research in this area.
At this occasion of the approval of biotin as a food additive, it
is expected that the importance of biotin will be reviewed, and
that biotin supplement developed based on the latest research results
will
be available.
|
 |
 |
| The alpha-amino group of L-arginine
mediates its antioxidant effect (S.Wallner et al. Eur.
J Clin. Invest.2001, 31, 98-102) |
| |
|
L-arginine has been shown to reduce atherogenesis,
both in animal and human experiments. It affects the platelet aggregation
or the attachment of monocytes (leukocytes) to blood vessels, which
are essential steps in atherogenesis. Conventionally, the effect was
attributed to arginine's role as a NO (nitrogen monoxide) precursor,
which results in an increased NO production and therefore leading
to functional improvement of vascular endothelium. However, our recent
study has shown that administration of external arginine delays the
internal peroxide eliminative action and the cell-mediated NO degradation,
and also decreases lipoprotein oxidation which is induced in the presence
of copper.
Furthermore, vitamins C and E also improve the vascular endothelium
function and inhibit atherogenesis. Therefore, it is considered that
not only the NO production but also the antioxidative effect of arginine
is involved in such inhibitory effect.
The antioxidative effect of arginine, characterized in the lipoprotein
oxidation model, may play a role in atherosclerosis resistance. Furthermore,
copper ion is involved in the initiation of LDL oxidation by binding
to ApoB-100 (the main protein in LDL (low-density lipoprotein)) at
a specific saturated state. It is believed that free radicals penetrate
and diffuse into lipid layers from this oxidation initiation point
by transferring from surface to surface of lipid particles.
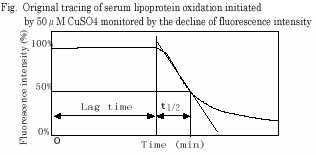
While monitoring the serum lipoprotein level using fluorescent probes,
the antioxidative effects of L-arginine, N-alpha-acetylarginine and
vitamin E in combination with arginine, were determined after the
free radical generation induced by copper (CuSO4) or AAPH (2,2'-acobis(2-amidinonpropane)
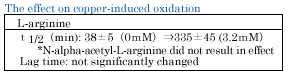
hydrochloride). The propagation rate of copper-induced lipoprotein
oxidation increased in a dose-dependent manner by L-arginine treatment
but not by N-alpha-acetylarginine treatment.
The propagation of copper-induced lipoprotein oxidation was represented
by a reduction in the fluorescence level. Concerning the time required
for this, the time required to reach half of the initial level (t
1/2) increased by L-arginine treatment in a dose-dependent manner,
but not by N-alpha-acetylarginine treatment. |
 |
|
|
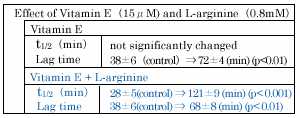
Vitamin E and L-arginine show different effects on copper-induced
oxidation, the former increasing only lag-time, the latter increasing
only propagation rate, and do
not have reciprocal effects.
|
 |
 |
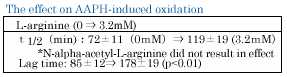
| In contrast to copper-induced oxidation, L-arginine
increased the lag-time of AAPH-induced lipoprotein oxidation, with
no effect on the propagation rate at physiological concentrations.
Again, N-alph-acetyl-arginine did not show any antioxidation effects. |
 |
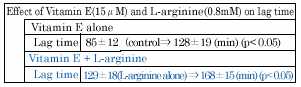
| This suggest that the effect of the combination of L-arginine
and vitamin E on the lag time of AAPH-induced lipid peroxidation was
additive rather than synergistic. |
 |
| Our experiments provide further evidence,
that mechanisms other than serving as a substrate for the NO-synthase
could be involved in L-arginine's antiatherosclerotic effect. In addition,
our experiments clearly show, that the antioxidant effect of L-arginine
is due to a chemical moiety differenr from that necessary for NO biosynthesis. |
|
|
|
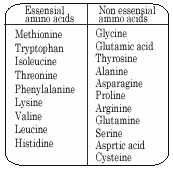
| Basic knowledge on amino acids |
Proteins are important components of our body accounting
for about 20% of our body weights, forming the cells, hormones and
enzymes in our organs and muscles. Approximately 500 kinds of amino
acids have been found in the nature. Among these, merely 20 kinds
of amino acids are used in various combinations to form 100,000 kinds
of proteins.
Among the 20 amino acids, eleven can be synthesized in our body to
make up for their deficiencies, while the other nine must be taken
up from our meal. The former eleven are called nonessential amino
acids, while the latter are called essential amino acids.
Within our bodies, some amino acids are re-synthesized into proteins,
while the others are stored within cells or blood, which are called
free amino acids. Most free amino acids, including the nonessential
amino acids, are extremely important for maintaining our lives. |
 |
|