|
--The Brain's Abnormal Permeability to Food Components Caused by Vitamin C Deficiency-- Professor Mieko KAWAMURA
There have been many experimental studies on the relationship between
nutrition and the development of the brain. As for the stage in which brain
cells increase in number and that in which the cells enlarge, the effects
of undernutrition on brain functions have been studied mainly in terms
of energy metabolism and such nutrients as proteins, lipids, and vitamins.
On the other hand, as for fully-developed brains, various studies have
been conducted on the functions of the neurotransmission system which represent
brain functions. Through these studies, it is becoming clear that changes
in the functions of neural receptors can be induced not only by such physiological
factors as aging and gender but also by various dispensable foods.
Ascorbic acid (AsA) is a necessary nutrient for the brain which
passes through the barriers of the brain. As for the distribution of AsA
after the entrance to the brain, it has recently been reported that AsA
is not distributed evenly but localized in rats' brain. Then, does a change
in the pattern of food intake, i.e. living on a diet deficient in AsA,
cause any change in the distribution of AsA in the brain or in brain functions?
We are measuring the continuous change of the amount of AsA in the brain
of ODS rats, which are genetically incapable of synthesizing AsA, when
deficient in AsA and in the process of recovery. Growing ODS rats fed with
AsA-deficient food develop rough fur, which is an AsA-deficiency symptom,
in the second week. However, the time required before the amount of AsA
in tissue drops because of AsA deficiency is different in different tissues.
For example, such a drop is seen in half a week in the blood serum and
in one week in the liver. In the whole tissue of the cerebral cortex, the
change is moderate during the first one and a half weeks, and in the third
week the drop reaches 3% of that of the controls. In the intercellular
part of the cerebral cortex, the drop reaches 22% of that of the controls,
followed by a more moderate decrease. In the brain, as the drop of the
amount of AsA is more moderate in the intracellular part than the intercellular
part, some regulatory mechanism is likely to be involved.
In the above, I have taken AsA as an example of a nutrient which
passes through the BBB and introduced changes in the brain caused by a
change in the pattern of AsA ingestion. On the contrary, there are reports
in which changes in the function of the BBB are presumed to be induced
by nutrients which cannot pass the BBB. It has been known that a type of
vegetable amino acid which stimulates nerves has this effect as an agonist
of glutamic acid through animal experiments in which this substance was
administered directly to the brain. However, usually the substance does
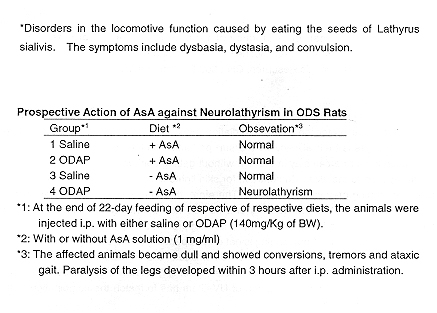
not enter the brain because of the BBB. AsA-deficient rats abdominally
administered this amino acid showed lathyrism*, or neural symptoms, whereas
the controls do not show any change. Rats with the neural symptoms stop
their locomotion and tremor, paralysis of legs, etc. are observed. These
symptoms are presumed to be caused by the entrance of the neuro-stimulating
amino acid to the brain because of damage or change in the function of
the BBB induced by AsA deficiency. Such symptoms are actually found in
people in poor nutritional conditions in developing countries after they
eat beans grown for food and decoration and containing this substance.
The causal substance of lathyrism contained in the beans, 3-N-oxyalyl-1,2,3-diaminopropane
(ODAP), has a direct effect on neural receptors, resulting in the liberation
of zinc and the formation a strong chelate with this zinc, causing zinc
deficiency. Zinc is liberated at glutamin-dependent synapses upon neural
stimulation and is believed to regulate the level of neurotransmission
by glutamic acid. Patients with lathyrism show decrease in zinc levels
in the blood. It is likely that excessive neurotransmission occurs in a
zinc- deficient brain, causing functional disorders.
In the above, I have introduced part of our study showing that AsA deficiency
causes not only disorders in the neurotransmission system but also morphological
changes in neurons, and that the same deficiency causes cerebrovascular
damage which induces a change in the BBB function, resulting in changes
in the permeability to substances entering the brain.
|
|
|
F. Hoffmann-La Roche Ltd, Vitamin and Fine Chemicals Cosmetic Research, CH-8600 Duebendorf, Switzerland
Introduction
Method
Irradiation conditions
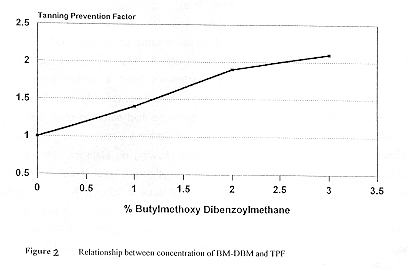
Calculation of Tanning Prevention Factor (TPF)
Discussion
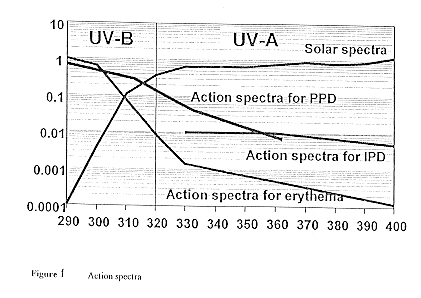
Tanning prevention is different from general sun protection. Normal
sun protection is assessed on its efficacy to prevent an erythema. As
the action spectra for tanning is different to the action spectra for erythema,
so is the optimum filter combination different for the two purposes. It
has to be taken into account, that of the total UV-radiation reaching the
earth surface only about 20% (21.1 W/m2) is UVB-radiation and 80% (85.7
W/m2) is UVA-radiation. The protection from UVB-radiation is expressed
in the SPF. Various methods are available and also comparable, since all
the products use defined solar simulated irradiation spectra and differ
mainly in the statistical treatment of the results, the number of volunteers
and the size of the application fields. Similar to the SPF we developed
a method to quantitatively assess the protection from UVA-radiation and
therewith the efficacy of tanning prevention on skin.
Conclusion
|
 |
|
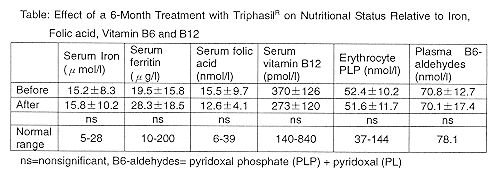
(from Nutritional Concerns of Women) Impairment of Folic Acid Status
Impairment of Vitamin B12 Status
|
 |
|
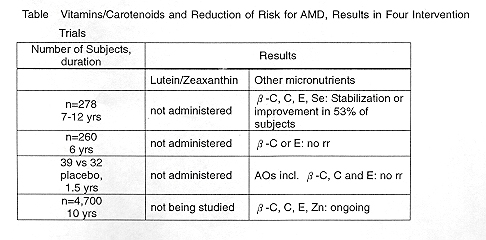
(from Nutritional and Environmental Influences on the Eye)
INTERVENTION TRIALS
|
 |