
|
Vitamin Levels of People of Advanced Age
The University of Miyazaki, Miyazaki Aiwa Hospital, and Miyazaki University of Medicine Yoshifumi Tomita, Noboru Saito, and Minoru Hamada Abstract:
Japan's aging society and pride in Japanese longevity
have made the health problems of people of advanced age important not only
for enjoying rich quality of life in our old age but also for reducing
the medical and nursing costs, which are rapidly putting pressure on the
financial situation. In order to maintain our health and prevent disease,
adequate intake of nutrition is important. However, people of advanced
age are generally deficient in vitamins, especially in vitamins A, B1,
B2, B6, B12, C, and D 1)* Although there are many causes for this problem,
the main cause is not that their vitamin intake is insufficient but that
the amount of food they eat at each meal is too small. The necessary energy
allowance depends partly on the activity level of each person, but it is
true that it generally decreases sharply with age: compared to people in
their 50s, the necessary energy allowance is 80 % for those in their 60s,
70 % for those in their 70s, and 65 % for those in their 80s.However, there
is little change in the allowances of Vitamins. Therefore, their meals
cannot be reduced simply in quantity, but must be considered in terms of
quality. In many cases, people of advanced age are unable to eat appropriately
due to disabilities in the limbs as well as disorders in mastication and
swallowing. Many people of advanced age suffer from deterioration of such
functions as digestion, absorption and metabolism due to aging. The rate
of those who are receiving medical treatment is high in these people, and
numbers of them are hospitalized. The main causes of hospitalization are
diseases in the circulation system and mental disorders. These people's
vitamin levels are affected not only by these diseases but also by medical
treatment. For example, cerebrovascular diseases cause eating disorders,
lack of appetite due to lack of exercise, and lack of appetite and nausea
due to treatment and medication.The patients are susceptible to infection
because of the deterioration of the defense system, and when they are actually
infected, their demand for vitamins increases and the vitamin levels in
the body decrease. The administration of antibiotics then changes the intestinal
flora, resulting in an inability to sufficiently produce vitamins which
humans can usually provide for themselves. Diuretics accelerate the loss
of hydrosoluble vitamins. Anticonvulsants, often used for cerebrovascular
disorders with diffused lesions, affect the metabolism of vitamins by deteriorating
liver and kidney functions. In the case of vitamin A, retinobbinding protein
(RBP), which is synthesized in the liver, determines the shift of the vitamin
from the liver to the blood. Therefore, disorders in liver and kidney functions
directly affect the vitamin A level in the blood.
|
|
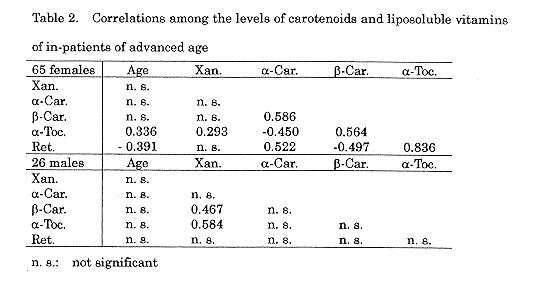
In this paper, we have introduced some study results on liposoluble
vitamins, 15-carotene, and carotenoids, but hydrosoluble vitamins are no
less important in relation to geriatric diseases. Similar studies should
be done by more researchers, and it is necessary to investigate the vitamin
levels of people of advanced age in relation to various diseases. It is
particularly important to follow up relatively large populations over a
long period, starting from an early age until an advanced age, including
investigation into life styles.
References:
|
|
 |
| CONFERRENCE REPORT
LC-PUFA in Focus ISSFAL Meeting |
| We publish here the second part of ourreport from the meeting of the
International society for the Study of PattyAdds and L4ids (1SSFAL), 2-5
June.
Protection against sudden cardiac death How does dietary fish protect men against sudden cardiac death? A good surrogate measure of risk of anthythmia and death is a reduction in heart rate variability (HRV). Jeppe Christensen and colleagues in Denmark have already shown that omega-3 supplements increase HRV in patients who have already had a heart attack, and in those with chronic renal failure. But is it effective in healthy persons? Their current research shows that it appears to work in men, but not in premenopausal women. Sixty volunteers, male and female, average age 38, were given long-chain polyunsaturated fatty acids (LC-PUFA) as a low dose (2 g pmega-3 LC-PUFA daily), high dose (6.6 g 4), or placebo.At the start and finish of the 1 2-weck period, heart rate variability was established by 24-hour monitoring, and omega-3 levels were measured in granulocyte membranes. Though no effects were found in the women the results for men were impressive: lowdose supplementation increased HRV by 3 milliseconds, and high doses by 12 ins, and membrane LC-PUFA levels also rose. The findings of this intervention study have been supported by research with animals. Drs A Leaf and JX Kang, Harvard Medical School, gave intravenous infusions of concentrated omega-3 oils, including ecosapentaenoic acid (EPA), docosahexaenoic acid (DHA), and alpha-linolenic acid (ALA), immediately before compressing a coronary artery. This manoeuvre produces ischaemia, which In turn induces arrhythmia. The LC- PUFA significantly prevented fatal arrhythmias by electrically stabilizing myocytes. The treatment shifted steadystate inactivation potentials by inhibiting Na+ and Ca++ currents. EPA,DHA and ALA were all 100% effective (in 46. 32 and 5 animals resoectivelvi. |
Arachidonic acid (AA) was less effective; out of 48 dogs, it had good
results in 18, a slowing of arrhythmia in 16, and no change in the remainder.
Saturates and monounsaturates had no effect either way. "We are ready"said
Dr Leaf, "to perform the randomized clinical trial needed to learn if what
we find in the laboratory will save lives and benefit humans, as preliminary
data suggests." Now that cholesterol-lowering drugs are available to treat
patients with heart disease, do they need dietary recommendations or other
intervention? Professor A Nordoy, Tromso University, pointed out that the
statins have been available for only a few years, while our knowledge of
the relationship between dietary fatty acids and coronary heart disease
(CHD) has been accruing clinically experimentally and epidemiologically
for half a century. We know that saturated fats seem to favour atherogenesis.
and that monounsaaturated fats may inhibit the development of arterial
lesions.LC-PUFA, however, of the omega-3 and omega-6 families, may reduce
the risk of CHD. Their concentration in the dietis crucial to cardiac health.
Nordoy considers there is sound evidence for supplementing statins with
dietary fatty acids. The seven countries. study seemed to suggest that
living in. Northern Europe involves cardiovascular hazards: raised cholesterol
levels can be more dangerous in a cold climate. On the other hand, in wartime
Norway there was plenty of fish and a shortage of saturated fat, and the
cardiac death rate fell. In fish-eating areas (such as Japan. and in Eskimo
territory) there is no visible effect in supplementing the diet with fish;
but in non-fish-eating areas, even a small amount of fish in the diet is
protective.
flesh, fish or cereal oil? LC- PUFA increase platelet EPA levels in humans. They can be obtained from plants, fish, or even lean red. Meat Which is the best source? Pd Sinclair and colleagues of RMFF University, Victoria, Australia, have found that fish is better then either lean meat, cereal oil, or flaxseed oil. In an earlier study by Mann et al in 1997 a group of 23 adult omnivores were given either 350 g of Jean red meat daily, or 135 g Atlantic salmon daily. After a fortnight,the platelet EPA levels of those eating salmon had risen by 1.3%, while those on meat had a rise of only 0.2%. The Australians now supplement this data with a comparable study on 17 vegetarians. All had 2 weeks of a diet high in ALA, and then they were given either rapeseed oil and rapeseed margarine (Canola) or flaxseed oil and fiaxseed margarine. |
Those on rapeseed products had an 0.1% EPA rise, while those on flaxseed
products had an 0.3% rise. After analyzing the EPA and ALA levels of the
diets, they conclude that "70 mg/day of EPA was more effective than 3.7
g of ALA, and almost as good as 15.4 g of ALA in raising platelet EPA levels"
Dr Peter Howe and Dr Peter Clifton,CSIRO, Adelaide, Australia, compared
two fish oils: Nu-Mega, which is particularly DHA-rich, with MaxEPA, which
is EPA-rich. Thirty volunteers took a 1 gram capsule daily for 6 weeks,
had a 4-week wash-out period, and then took the other capsule for 6 weeks.
MaxEPA raised EPA by 350%,and DHA by 63%. Nu-Mega raised EPA by 140% and
DHA by 130%. Despite these differences, both reduced plasma triglycerides
by 26% and thromboxane production by 40%. This suggests that DHA is relatively
more effective than EPA Neither product caused any change in blood pressure
in these mildly hypertensive volunteers, but MaxEPA was better at lowering
interleukin-1 -beta.
Points from posteis MaxEPA was compared to olive oil (the control) in rats. It lowered plasma triglycerides by 75%, and cholesterol by 30-50%. Clotting was 30% slower, via action on factors II, VII, VIII, IX and X. When thrombus formation was experimentally induced, the thrombi were smaller and fewer compared with olive oil. (Andriamampan-dry, INSERM,Strasbourg.) LC-PUFA reduced the blood pressure of old rats with genetically-determined spontaneous hypertension. At 53 weeks of age the animals were given a concentrated preparation containing GLA. EPA and DHA, and were compared with untreated controls given normal rat pellets. After 5 weeks, BP was 159mm Hg in treated animals and 189mm Hg in controls (Germain,Universite de Bourgogne). When female rats were fed a diet high in saturated fat - intended as the rodent equivalent of a Western human diet - before, during and after pregnancy, their pups showed a 33% reduction of DHA levels. At 15 days, their femoral arteries, when studied invitro, showed a significantly reduced response to acetyicholine, and reduced sensitivity to a nitric oxide donor.(Koukkou et al, St Thomas's Hospital,London). |
|
LC-PUFA status In pregnancy and lactation Dr Gerard Hornstra, Depaitment of Human Biology, Maastricht Universityr
Netherlands, considered the relationships between maternal and foetal essential
fatty acids (EFA). Circulating levels of long-chain polyenes (LCP) increase
by 40% or more during pregnancy. This is not due to a change in diet, and
there appears to be little change in EFA desaturation and elongation. This
leaves two possibilities: that pregnancy causes a functional re-routing
of LCP from 'fuel' to 'building bricks; or that LCPs are mobilized from
maternal stores. If the latter is the case, this would explain why first-time
mothers and their babies have higher DHA levels than multigravidae and
their children. The more children there are in a family, the lower their
LC-PUFA levels. Moreover, twins and tnplets have lower levels than singletons,
as has been shown by measurement in umbilical cord plasma and tissues.
This difference is even more marked in umbilicar tissue levels than in
umbilical plasma. Since LC-PUFAs will get into cord plasma before reaching
cord tissues, this suggests, says Hornstra, that placental LC-PUFA transfer
gradually improves during pregnancy. This implies that specific adaptations
develop to transfer LC-PUFAs from mother to foetus. However, recent evidence
suggests that maternal diets have, typically, a less than optimal omega-3
/ omega-6 ratio, and this may compromise optimal foetal development
|
subsequently breast-fed their babies, and 10 did not Their
average age was 30. All carried their babies to term. Otto and colleagues
collected (or plan to collect) measured maternal plasma lipids at 36 weeks
of pregnancy, on the 2nd and 5th day post-partum, and at 1, 2, 4, 8,16,32
and 64 weeks post-partum. They were able to present results for up to 16
weeks post-partum, and which indicate that maternal DHA status continues
to decline after delivery, the reduction being more pronounced in lactating
mothers. The mothers who subsequently breast-fed had, initially, higher
DHA levels than the non-breastfeeders:4.71% by weight of total fatty adds,compared
with 4.07% Within a week of delivery the two groups were substantially
the same, and by week two the lactating women had noticeably lower levels,
3.71% compared to 3.33%. Between week 4 and week 8, levels were down to
non-pregnant levels in both groups. But from week 2 onwards. the two groups
diverged rapidly: by week 8 the lactating mothers were down to 2.55%, compared
with 3.37% (P<0.05) in non-breasifeeders. By week 16, the figures were
2.62% coinpared with 3.43% (P<0.01). In all,between 36 weeks of pregnancy
and 16 weeks post-partum, the DHA levels of lactating mothers fell by nearly
45%, while those who did not breastfeed showed a drop of only 15%. Drs
Otto and Hornstra therefore advise supplementation with DHA for breast-feeding
mothers.
Breast-feeding and development hree posters by C Agostoni, F Marangonia et at, San Paolo Hospital and Milan University Pharmacology Department, looked at various aspects of breast-feeding. In the first study, longer breast-feeding was found to correlate with better developmental scores in a cohort of healthy term babies who were exclusively breastfed for 3 months and at least partly breast-fed for 6, 9 or 2 months. The authors suggest this is due to the supply of fats contributing energy and/or affecting the composition of brain membranes. A total of 95 babies met the inclusion criteria and 44 completed the 12-month study. Smokers had fattier colostrum milk -2.0 versus 1.5 g/dL - than non-smokers, and in particular there was more omega-6 LC-PUFA. But by 1 month |
the situation was reversed, and non-smokers had more EFA,
especially omega-3. 44 mothers entered the study and 22 completed it; of
the original 44.31 were non-smokers, while 13 smoked 5-15 cigarettes a
day; six of the latter continued to smoke 1-2 cigarettes a day during pregnancy.
Lipid balance improved in women who exclusively breast-fed for three months.
They experienced a 30% lowering of plasma lipids, total cholesterol, low-density
lipoprotein (LDL),and triglycerides. Their levels of highdensity lipoprotein
(HDL) rose. Their plasma omega-6 levels rose, and omega-3 levels declined.
In their milk,triglycerides and 18-C PUFA rose. The results suggest that
18-C PUFA are directly transferred from plasma to milk, while long-chain
PUFA concentrations could be modulated by the mammary gland.
Healthy Third World babies Healthy Third World babies (defined as babies who weigh at least 2,750 grams at birth, have no adverse obstetric, nutritional and paediatric complications,and are breast-fed) may well have a better DHA status than Westem babies, according to a poster presentation by Professor Michael Crawford et al. This advantage arises from the relatively low fat content of material diets - InThailand only 16% of dietary energy comes from fat compared with 40% in the Western diet But is the difference reflected in the quality of breast milk? To find out the investigators compared the DHA content of Eastern versus Western breast milk Mothers from Thailand and Europe were matched for age and parity and their milk sampled at intervals. Eighteen weeks after delivery, when the milk is mature, the DHA level of Thai mothers' milk was 0.57% of total fats, compared with 0.33% in Western mothers. This confirms previous studies, which have shown a level of 0.6% in Chinese mothers, compared with 0.15% in Western mothers. Crawford and colleagues conclude that the high-fat Western diet is associated with reduced levels of DHA and, further, that levels closer to 0.9% total omega-3 metabolites (0.36 g/Kg/24 hours or 0.11 g/Kg/24 hours) would be more appropriate for infant formulae". Several expert committees (FAO/WHO 1994,ISSFAL 1994) have recommended that infant formula should have the same percentages of AA and DHA as breast milk, but some formulas contain none whatsoever, or only trace amounts, he noted. |
|
DIIA formation Inadequate Work on cats indicates that the last desaturation step in forming DHA takes place in the brain rather than the liver; it is reasonable to suppose that the same is true in humans, suggested Dr Norman Salem, Laboratory of Membrane Biochemistry & Biophysics, National Institute of Alcohol Abuse & Alcoholism, USA. In adults, DHA formation is decreased when dietary intake of EPA/DHA is increased; therefore the extent of DHA/AA synthesis may be a reflection of dietary inadequacy. In newborn babies, the data suggest that the amount of DHA formed in the body may not be adequate to supply developmental needs. "Therefore under customary dietary conditions, preformed DHA must be supplied" Children suffering from malnutrition have poor essential fatty acid (EFA) levels, and standard medical treatment fails to replenish this with sufficient speed. Drs Virgilio Bosch, Sonia Bomo and Maria Reymundez (Lipidology Section, Central University, Caracas, Venezuela) studied 32 malnourished children under 5 and compared them with 22 adequately-nourished controls. The children were rated using WHO criteria; the degree of malnutillion was mild in 10, moderate in 6, and severe 16. The ratio of non-EFA/EFA was 1.53 in controls, but in the malnourished groups it was 1.85, 2.47 and 2.27 respectively. The malnourished children had higher blood levels of mead, palmitic and oleic acids. A marked EFA deficiency is dearly a common feature of even mild cases of malnutrition. These children have usually been breast-fed for only a month, as the mothers have to return to work. In Venezuela the routine treatment for these children is a dietary supplement of corn oil and animal protein, but this may lead to unduly slow replenishment of omega-3 PUFA. They consider that specific additional intervention is needed so that EFA is rapidly replenished in all tissues, adding that is particularly important if we consider than one of the major complications of malnutrition is immune incompetence." Infants with phenylketonuria (PKU) are another group for whom supplementation should be considered. This inborn error of metabolism causes severe mental retardation if it is not treated by a strict diet. Dr Houwelingen, Maastricht University Hospital, evaluated the EFA status of 9 PKU sufferers aged 6 months to 25 years. Each was matched to two controls. PKU sufferers were found to consume significantly less fat, including omega-3 and omega-6 long-chain polyenes. Their plasma and erythrocyte were low in omega-3 and relatively high in omega-6." We conclude that, due to a low dietary intake of omega-3 LC-PUFA fatty acids, PKU subjects have a low omega-3 LC-PUFA status. On the basis of these results supplementation of the PKU diet with omega-3 LC-PUFA fatty acids should be considered". |
children under 5 and compared them with 22 adequately-nourished controls.
The children were rated using WHO criteria; the degree of malnutil- lion
was mild in 10, moderate in 6, and severe 16. The ratio of non-EFNEFA was
1.53 in controls, but in the mal- nourished groups it was 1.85, 2.47 and
2.27 respectively. The malnourished children had higher blood levels of
mead, palmitic and oleic acids.
A marked EFA deficiency is dearly a common feature of even mild cases of malnutrition. These children have usually been breast-fed for only a month, as the mothers have to return to work. In Venezuela the routine treat- ment for these children is a dietary supplement of corn oil and animal pro- tein, but this may lead to unduly slow replenishment of omega-3 PUFA. They consider that specific additional intervention is needed so that EFA is rapidly replenished in all tissues, adding that is particularly impor- tant if we consider than one of the major complications of malnutrition is immune incompetence:' Infants with phenylketonuria (PKU) are another group for whom supplementa- tion should be considered. This inborn error of metabolism causes severe mental retardation if it is not treated by a strict diet. Dr Houwelingen, Maastricht University Hospital, evalua- ted the EFA status of 9 PKU sufferers aged 6 months to 25 years. Each was matched to two controls. PKU suffe- * rers were found to consume signifi- candy less fat, induding omega-3 and omega-6 long-chain polyenes. Their plasma and erythrocyte were low in omega-3 and relatively high in omega- 6. Vk condude that, due to a low diet- ary intake of omega-3 LC-PUFA fatty acids, PKU subjects have a low omega-a LC-PUFA status. On the basis of these results supplementation of the PKU diet with omega-3 LC- PUFA fatty acids should be considered" |
Neurological disorders
DJ Kyle (Martek Biosciences) with Tufts University, Boston, investigators, assessed the blood DHA levels of 1,188 elderly people, mean age 75 years. Those in the bottom half of DHA levels had twice the incidence of Alzheimer's (11 versus 5) at the time the blood sample was taken. Of those without Alzheimer's, those in the bottom half had a 60% greater likelihood of developing it in the subsequent 10 years (P<0.05). It is important for the elderly to maintain adequate levels of serum DHA through the consumption of fish or dietary supplements, they concluded. Dr S. Connor was the main author of a poster showing that higher plasma omega-6/omega-3 levels were associated with dementia and death in the elderly. This team from Oregon Health Sciences University used a sub-sample of the Oregon Brain Aging Study. Data were collected in 1992-3 and analyses done in 1998. Complete data were available for 49 women and 36 men. Of these, 14 had developed dementia and 11 had died. Elderly people with cerebrovascular dementia show improved mental function after DHA supplementation, according to a poster presentation of Takashi Terano of Chiba Municipal Hospital, Japan. Twelve elderly people, average age 83. with symptoms of dementia, were given 720 mg DHA a day in 6 capsules; 12 other dements were registered as a control group. In the supplemented group, dementia scores were significantly better than in controls after 6 months (p<0.05). Red blood cell deformability also improved, but platelet aggregation was unchanged. Elderly people have low LC-PUFA levels in their blood and would benefit from dietary supplementation, according to a poster presentation by E Polichetti et al from the INSERM department of human nutiltion, Gerontology Centre, Marseilles. DHA levels in red cells and plasma were measured in 47 men and women, average age 80. Compared to controls levels of most PUFAS were reduced: DHA was down by 25%. |
|
|
| B Vitamins: Essential in Enety Metabolism. because they generaily function
as part of critical enzymes that are Involved with the conversion of carbohydrates,
fats and proteins to useful energy Therefore, requirements for some B vitamins
are tied to eneay intakes. For example, the Recommended Dietary Allowance
(RDA) for niacin is 6.6 mg/1000 calories consumed, the RDA for riboflavin
Is 0.6 mg/1000 calories consumed, and the IIDA for thiamin is 0.5 mg per
1000 calories consumed, but not less than 1.0 mg/day. Similarly, vitamin
B6 requirements are based on estimated protein intakes; die RDA is 1.6
mg/day for women and 2.0 mg/day for men, or approximately 0.016 mg/gram
of protein consumed per day. B vitamins are also involved in the synthesis
of DNA and RNA and the functioning of the nervous system.
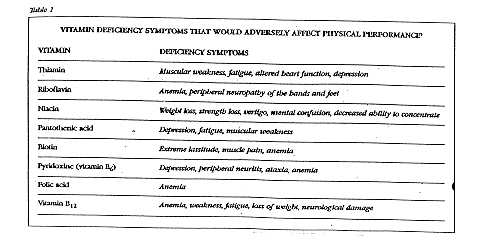
Because of their essential roles in energy generation, nerve function and the formation and maintenance of body support structures (muscle and bone),"lt is virtually certain that a deficiency or suboptimal status of any vitamin will, at some point, impair physical performance"' This is particularly true if dietary intakes of several vitamins are suboptimal simultaneously. Frank deficiencies of vitamins result in a wide variety of adverse symptoms that would diminish playsical performance (Table 1). In addition, there .is evidence that more subtle vitamin inadequacies may have an Impact. For example, a combined marginal deficiency of thiamin, riboflavin and vitamin B6 caused a decrease in physical performance within a few weeks Some research has shown that exercise is most likely to affect riboflavin status when a training regimen is unaccustomed or sporadic. Five separate studies have reported that exercise increased riboflavin requirements in untrained women; in contrast, no evidence for an increased requirement was observed in two studies with trained women. It is suggested that perhaps riboflavin needs are increased at the beginning of an exercise program but that adaptation may occur in trained subjects, allowing them to maintain riboflavin status on intakes approximating the RDA.' |
Whether this will occur for other vitamins is not known.
Most physically active people consume enough food to fulfill both their energy and micronutrient needs, but there are some cases where this may not be the case. Physically active people who also restrict calories are likely to have inadequate intakes of several vitamins. Athletes who restrict their food Intake to maintain low body weight, as is often the case among those Involved in gymnastics, dancing diving, figure skating and college wrestlIng, may be at risk for inadequate vitamin intakes. Even recreationaI exercisers who diet for weight control may be at risk. For example, the combination of dieting plus moderate exercise 2 1/2 hours a week of aerobics - was shown to increase the requirement for riboflavin. Exercise and Oxidatfr'e Stress. Performance of strenuous physical activity can increase oxygen consumption by 10 to 15-fold over rest. This in turn produces oxidative stress through the generation of free radicals and increased lipid peroxidation in skeletal muscle cells~ Exercise can also generate free radicals by other means, including increased production of epinephrine and other catecholamines that can produce oxygen radicals by autoxidation production of lactic acid that can convert a weakly damaging radical (superoxide) into a strongly damaging one (hydroxyl); and the immune response to muscle damage as a consequence of overexertion, which can lead to lipid peroxidatlon of membranes and an increase in macrophages and white blood cells in damaged muscle. In general, there Is evidence that strenuous exercise can increase lipid peroxidation, as measured by biochemical markers of free radical production. In particular certain byproducts of lipid peroxidation are detectable in the blood (plasma MDA or malondialdehyde and conjugated dienes) and in the breath (expired pentane); however these mea- surenients have been criticized as being imprecise. Evidence for increased oxidative stress is also suggested by the fact that regular physical training appears to enhance antioxidant status,as measured by elevated levels of vItamin E and antiox- idant enzymes in highly trained runners." |
 |