|
[Abstract]
1. Introduction Macrophages produce and release nearly 100 different chemical mediators such as prostaglandins, leukotrienes, PAF, reactive oxygen, and monokines in response to various stimuli, playing a major role in the inflammatory response and homeostasis. Among the mediators, monokines such as IL-1, .IL-6, IL-8, TNF-α and MIF form a cytokine network with vascular endothelial cells, smooth muscle cells, T cells and others, functioning as major intercellular messengers in the inflammatory; immune and other responses. On the other hand, it has been indicated that vitamin E not only has an antioxidant function but also a "beyond antioxidant function", which is made up of a variety of physiological activities through cellular metabolism or genetic modulation, through which the vitamin participates in the immune and inflammatory responses. However, the mechanism of these activities of vitamin E has not yet been elucidated in detail. In order to make this point clear, we investigated the relation between vitamin E and macrophage monokine production in terms of the modulation of macrophages with the vitamin. |
| 2. Monokines and Inflammation
The inflammatory cytokines TNF-α and IL-6 are monokines mainly
produced by monocytes and macrophages. These monokines are found in high
concentration in the arterial synovium of people with rheumatoid arthritis.
This suggests that macrophages play a major role in rheumatoid arthritis.1)
On the other hand, it has been indicated that TNF-α causes injury in vascular
endothelial cells through promoting procoagulant activity; production of
prostaglandins and PAF, and leukocyte-endothelial cell adhesion, thus playing
an important part in the development of arteriosclerosis.2) Recently, macrophage
migration inhibitory factor (MIF) has been noted as a monokine that promotes
TNF-x production.3) Although MIF was originally discovered in vitro as
a cytokine that inhibits macrophage migration, recent reports have shown
that MIF attracts macrophages to inflamed tissues, causing inflammatory
and immune responses, and notably has a close relation with the delayed
hypersensitivity.
|
| 3. Vitamin E and monokines
W We have studied the relation between vitamin E and production
of O2 and PGE2 in terms of the functions of macrophages. As a result, we
have found that vitamin E not only has an antioxidant function in a stoichiometric
sense but also a "beyond antioxidant function", through which it inhibits
production of 02 and PGE2 through the modulation of macrophages. 7) Meydani
et al. have obtained the same result in invivo tests on vitamin E supply.
8) addition, they also reported that vitamin E promotes T cell growth and
IL-2 production through inhibition of PGE2 production, resulting in enhancement
of the immune response. However, the effect of vitamin E on the production
and the release of monokines such as IL- 6, TNF-α, and MIF has not yet
been fully elucidated. In order to make this point clear, we modulated
the macrophages of male Wistar rats (350〜400 g) by intra-abdominal administration
of 5 mg of vitamin E for 6 consecutive days and investigated the effect
on monokines. The result showed that the vitamin E content in the macrophages
of the control group was 1.2±0.4 ng/106 cells whereas that in the vitamin
E treated group remarkably increased to 384.4±76.1 ng/106 cells. Using
these macrophages rich in vitamin E, we then investigated the relation
between macrophage monokine production and vitamin E. The amount of secreted
monokines was quantified by ELISA using a specific antibody for each monokine
and sample were collected from the mediums of macrophages after 14-hr incubation
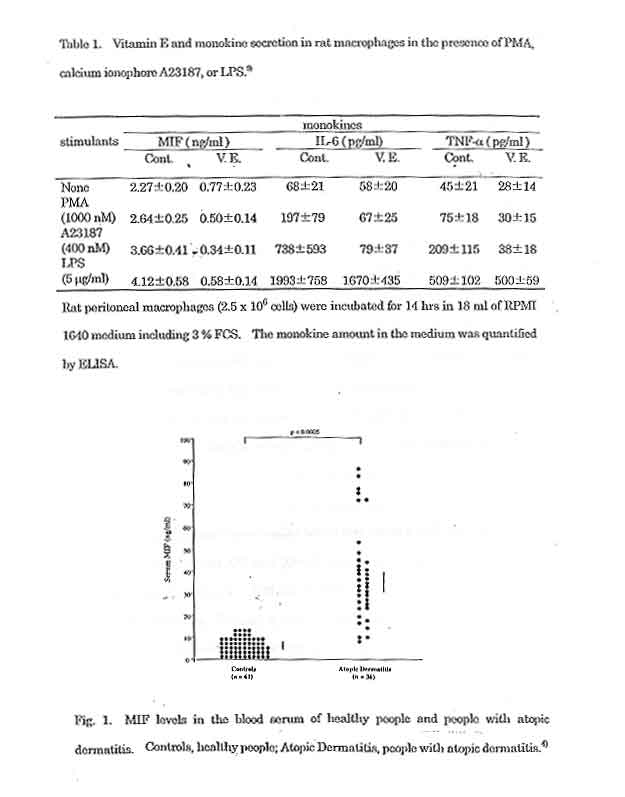
in the presence of various stimulants. *The results showed that the secretion
of MIF, IL-6 and TNF-α in the macrophages of the control group increased
in the presence of the following stimulants: the calcium ionosphere A23187,
phorbol myristate acetate (PMA), and lipopolysaccharide (LPS) (Table 1).
|
| 4. Conclusion
Monokines play a major role in the inflammatory and immune responses as protein mediators that participate in intercellular interactions. Therefore, regulation of monokine production leads to a novel therapy. In the present study, we investigated the relation between macrophage monokine secretion and vitamin E. As a result, we found that vitamin E has not only an antioxidant function but possibly a "beyond antioxidant function", through which the vitamin affects the intracellular signal transduction system through cell modulation. There are many points yet to be elucidated, and we expect an advance in the study on vitamin E as a clinical medicine from this new point of view. |
|
|
| Conference report
Role of Omega-3 LCPUFA in Lowering Triglycerides |
| ISSFAL, the International Society for the Study of Fatty Acids and
Lipids,meets about every two years; its third meeting was held in Lyons,
France, from 2-5 June. Here we summarize the main points of the symposium
on triglycerides; for which Professor Rudolph Riemersma (University of
Edinburgh, UK) and Professor William Harris (University of Kansas,USA)
were cochairmen.
Tnglycendes as a risk factor - epidemiology A link between elevated triglyceride levels and is chaemic heart disease has been known since the 1950s,Professor Michael Miller of the University of Maryland. USA, pointed out, but until 1980 the effect was attributed to cholesterol. The Framingham study showed that triglyceride levels per se were strongly correlated with coronary heart disease (CHD) risk, especially in women. These effects were often reduced after adjusting for other co-variables, but recent studies confirm that triglycerides are a risk factor in their own right. Hokanson & Austin 1996 showed that for each mmol/L rise in triglycerides, CHD risk rose by 14% in men and 37% in women. These figures are confirmed by Austin of Seattle's 1996 meta-anaysis of major trials, comprising 14000 individuals, evaluating fasting triglyceride, levels. The Copenhagen study of 000 healthy males, published in Circulation earlier this year, gave similar indications. Triglycerides also predict which patients will show disease on arteriography. Recent studies have also shown a correlation between triglyceride levels and carotid ischaemia.As doubling triglyceride levels raises risk by 50% in men and doubles it in women, this begs the question of what the recommended safe upper limit should be. A consensus panel of the US National Institutes of Health (NIH) in 1993 put it at 200 mg/dL, but Miller argued that it should be halved to 100. The NIH-recommended upper limits for triglycerides and cholesterol are both set at 200 mg/dL Yet the average US cholesterol level is around 200, twice the mean triglyceride level of around 100 (112 in men, 88 in women). Long-term follow-up of a group of |
cardiac patients in Baltimore showed that those in the lowest triglyceride
group had the fewest cardiac events, even when all other factors were adjusted
for, which adds further support to the argument for a lower cutoff point.
The next step should be to design an intervention study that will show
the effect on CHD incidence of lowering triglycerides.
Triglycerides as a risk factor - dinical view Professor Peter Schwandt of the University of Munich. Germany, pointed out that high plasma triglycerides not only double the CHD risk, but are a component of four other serious lipid disorders: * Chylomicronaemia syndrome, which may be associated with acute pancreatitis
and acute abdominal disease
Type II diabetes is also characterized by high triglyceride levels and micro-angiopathy, he observed. How should these disorders be treated? Prof. Schwandt suggested that the first clinical objective should be to lower serum triglycerides to under 200 mg/dL, except for diabetics, where the target should be to get below 150 mg/dL Weight reduction lowers LDL cholesterol, but, unfortunately, less so in diabetics than in controls. Advice to patients would include a better life-style, diet and exercise, reduced alcohol intake, and stopping smoking. Fish oil treatment may be included, particularly since it poses no risk to diabetic patients. Drug treatment, however,should be reserved for severe cases. |
Cardiovascutar disease incidence. Diet and lipids It is generally believed that a good diet,which may include fish oil, can reduce the risk of coronary heart disease, said Dr Riemersma, University of Edinburgh. However, it is often difficult to persuade the public to take dietary advice. Nevertheless, the effort is well worth while. The Dart Trial found that the advice to CHD patients to eat more fatty fish reduced the death rate over two years. This and the results of another dietary intervention study, the Lyons Heart Trial, are better than those obtained by drugs; simvastatin reduced serum cholesterol by 25% and CHD mortality by 32%. However, the evidence of the dietary intervention trials failed to make the same impact in the clinical treatment of patients as the drug trial, perhaps because diet trials are seen to be deficient in certain important aspects, including design and size. Can the Scots be persuaded to change their diet? Riemersma s research in Edinburg showed that all CHD patients showed a willingness to eat more fruit and wholemeal bread, and to cut down on potato chips. A group giving intensive dietary counseling (up to four hours per patient), including provision of recipes and free margarine, also changed the fatty acid composition of their diet, which was documented by objective tests. However, they baulked at eating more vegetables or drinking less fatty milk thus a total dietary change may perhaps be unrealistic. But it should be possible to conduct a large secondary prevention study,using a specially formulated margarine/oil or fatty acid supplements, and that would meet some of the criticisms of earlier trials. |
| Effect of Omega-3 LCPUFA on tri- glycendes in postprandial states
Triglyceride levels rise after meats, and the Physicians' Health Study showed that the amount of this rise was proportional to the amount of atherosclerosis present, and its progression. Dr Helen Roche, Trinity College, Dublin,Ireland, pointed out that the postprandial surge is worse in men than in non-menopausal women, increases with age, and in women becomes rapidly worse after the menopause. If the surge is plotted on a graph, the area under the curve is a direct predictor of coronary artery disease (CAD). Since it takes 4-6 hours to digest fats, and most people eat three or more meals a day, this means that lipids may be in an almost constant postprandial state. However, the triglyceride surge could be reduced by even quite modest amounts of fish oil, Dr Roche noted.The beneficial effect is dose-related; as the intake of the long-chain polyunsaturated fatty acids (LCPUFA) goes up,the level of postprandial triglyceridaemia goes down. She and Gibney gave 0.54 g eicosapentaenoic acid (EPA) and 0.36 g docosahexaenoic acid (DHA) daily, or placebo, for 16 weeks to two groups, matched for several parameters including fasting triglyceride levels. The result was a 20% reduction in fasting triglyceridaemia and a total 30% reduction in the area under the curve. Studies by other workers used different doses and duration of treatment, but all show comparable reductions in fasting triglyceride levels. Even at low doses there can be a reduction of 20-30%. Effects of EPA and DHA on plas- ma triglycendes Most studies of the effects of LCPUFA have been done using fish oil,
where DHA and EPA are of necessity given together; Dr Peter Weber, F.Hoffmann-La
Roche, took the discussion a stage further by considering EPA versus DHA
|
Controlled clinical trials comparing purified EPA with purified DHA
have shown that both PUFAs were consistently effective, both during fasting
and postprandially. Three studies using purified EPA, 2.7-4.0 g/day, lowered
triglycerides by 16 to 33%. DHA, 1.25-6 g/day, gives comparable results.lowering
triglycerides by 17 to 26%.The various studies show that there is also
a beneficial effect on lipid fractions. DHA may increase high-density lipoprotein
(H DL), and EPA is associated with a slight lowering of low-density lipoprotein
(LDL).
Metabolism of lipoproteins and effects of LCPUFA Professor William Harris, University of Missouri Medical Centre, Kansas City,USA. reviewed the effects of fish oil on human serum lipids and lipoproteins, as shown in well-designed, placebo-controlled, crossover or parallel studies. A recent and under-reported Indian study directly compared fish oil and mustard oil containing alpha-linolenic acid (ALA) against placebo. The two groups received roughly the same amounts of LCPUFA, but much higher volume was needed for mustard oil. However, it was nearly as good as fish oil in reducing angina and arrhythmias, heart failure, and total coronary events."This is the best study we've got to show that fish oils really do reduce coronary disease," Prof. Harris commented. Summary Safety aspects and recommendations Professor William Connor, Oregon Health Sciences University, Portland,USA,
closed the session with a review of safety aspects. He reminded the audience
that many indigenous peoples, including the Chinese living on the banks
of the Yangtse River, as well as the Eskimos and Indians living in northwestern
coastal areas, have consumed large amounts of fish oil for thousands of
years, in quantities as high as 50 g/day. That they have survived and flourished
is testimony to the safety of the much smaller doses now given to patients.
|
Nevertheless, there are theoretical risks, none of which have been
confirmed despite numerous clinical trials involving thousands of patients.
These are born out of some concerns.Eskimos have a high incidence of stroke,but
patients in clinical trials do not show any excess incidence. Studies have
failed to confirm fears regarding increased peroxide formation, possible
worsening of glycaemic control in diabetics, or carcinogenesis: the LCPUFA
in fact may slow the development of many cancers.
During the decades when cod liver oil was given to children to prevent rickets,no harm was ever shown. The tea-spoonful dose contains about 1.25 g of LCPUFA, "almost a therapeutic level", and fish oil capsules also have vitamin E, which prevents increased oxidation. Large doses of fish oil reduce the platelet count but not the total platelet volume, and there is no increased bleeding when patients given fish oil supplements undergo vascular surgery. In non-insulin-dependent diabetics. early studies showed decreased glycaemic control after taking fish oil.However, recent larger and better controlled studies have failed to confirm this. Moreover, diabetics benefit from the lowering of VLDL and triglyceride concentrations by fish oil. It is therefore logical anci practical to recommend fish oil and its constituent LCPUFAs, EPA and DHA, said Prof. Connor. It is especially logical to use purified "reparations, which contain 50% or more EPA and DHA, and therefore bring the required dose down from 6 g/day or more to 1-2 g/day.Fish oil should be the treatment of first choice for hypertriglyceridaemia, along with a low fat diet, exercise and weight reduction, he also commented, noting that it also lacks the risks of cholesterol-lowering drugs. Prof. Connor said he had observed in his own long dinical experience that patients will usually take their fish oils, unlike their cholesterol-lowering drugs. For the general population, a preventive approach should be based on consumption of fresh fish. "If you cannot get fish, don't like it, or are allergic to it, then take fish oil", Prof. Connor concluded. |
| Cardiovascular - Disease
Probucol and Multivitamins in the Prevention of Restenosis The long-term effectiveness of coronary angioplasty is limited by the high incidence of restenosis (recurrent narrowing of the treated artery). Since oxidizing metabolites generated at the site of angioplasty can induce chain reactions that may lead to restenosis, it has been suggested that antioxidants may prevent its occurrence. In a double-blind trial conducted at the Montreal Heart Institute, 317 patients with coronary artery disease were randomly assigned to receive one of the following: the antioxidant drug probucol; a coml)inaction of antioxidant nutrients (30,000 IU β-carotene, 500 mg vitamin C, and 700 IU vitamin E);both treatments; or placebo daily for one month before and six months after angioplasty. Follow-up angiographies showed that probucol therapy significantly reduced the rate of restenosis, but the antioxidant nutrients had no significant effect. The researchers who conducted the study speculate that the effect of probucol may have been due to some mechanism of action other than its antioxidant activity, since the nutrients, which are also antioxidants, had no effect.However, Hodis et al (1995) noted an association between supplementary vitamin E intake (100 IU or more daily) and angiographically demonstrated reduction in coronary artery lesion progression in 156 men receiving a cholesterol-lowering drug. No benefit of vitamin E was found in the placebo group,indicating that supplementation with vitamin E maybe of value as adjunctive therapy in patients who are receiving drug therapy for existing coronary artery disease. Jean-Claude Tardif, Gilles Cote, Jacques Lesperance et al,Probucol and Multivitamins in the Prevention of Restenosis after Coronary Angioplasty, N Engl J Med 337(6):365-372 (7 Aug 1997) [Reprints: Dr Gilles Cote, Research Center,Montreal Heart Institute, 5000 Belanger Street, Montreal PQ HIT 1C8 Canada] |
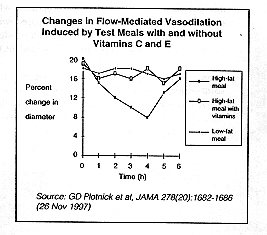
Vitamins C and E Block Fat-Induced Impairment of Endothelial
Function
Dietary fat may contribute to the causation of athero-sclerosis through impairment of endothelial function. Recent research has shown that consumption of a high-fat meal decreases endothelial function in the major arteries (as measured by flow-mediated vasodilation) for several hours. A low-fat meal does not have the same effect. Researchers at the University of Maryland have now conducted a study to determine whether pretreatment with antidxidant vitamins influences the effect of high- and low-fat meals on vasodilation. Healthy volunteers received either a high-fat (50 g fat, 900 kcal) breakfast, the same breakfast preceded by I g vitamin C and 800 IU vitamin E, or a low-fat (0 g fat, 900 kcal) breakfast. Tests of flow-mediated vasodilation in the brachial artery were performed at several intervals after the meal. As the graph on this page shows, the high-fat meal without vitamins produced a substantial change in vasodilation which was not observed after the low-fat meal. Pretreatment with antioxidant vitamins blocked this change, leading to a response almost identical to that seen with the low-fat meal. These results suggest that the short-term effects of dietary fat intake on endothelial function may be mediatedby an oxidative mechanism and that they can be prevented through supplementation with antioxidant vitamins.
|
|
10. What are the most important factors iifluencing sunburn and skin pigmentation? a. Intensity of light - Latitude - Altitude - Seasons - Time of day Length of exposure - Transmission through glass, clouds, water and clothes - Relexion off sand, snow and grass b. Skin types also influence sunburn and skin pigmentation. 11. Cosmetics containing AHA 's (alpha hydroxy acids are also known as fruit acids) are used to exfoliate surface skin cells. Is it important to avoid the sun when using these products? AHA containing cosmetics are used for skin renewal effects. AHA's stimulate the skin and as a result the skin becomes more sensitive to IJV rays. Cosmetics containing AHA's should either have a sunscreen as one of the ingredients or should be used together with a sunscreen with a minimum SPF of 9 or above on a daily basis. 12. Should dark skinned people use a sunscreen? The sun 'tans' dark skins as it does light skins. Dark skins will darken in the sun and therefore sunscreens can be an effective cosmetic for people who have a Phototype IV or V skin [See Table (Question 9) for clarification]. The tanning process in negroid skins can be reduced by high protection sunscreens which should be applied in the morning and at midday. |
 |
| Seminar Information
[The Latest Topics of Lipid Nutrition] supported by ILSI-Japan
1. Date: 28.Nov.1998 (Sat.) 13:30 17:30
4. For Registration
|