--Serum Carotenoid Levels of Oral Leukoplakia Cases-
Toru Nagao, Assistant Professor, The Second Department of Oral and Maxillofacial Surgery, Aichi- Gakuin University School of Dentistry
<Abstract>
As there is a risk of oral leukoplakia developing into oral cancer,
it is regarded as precancer. We measured serum micronutrient levels in
oral leukoplakia cases at inhabitant-based medical checkups for oral cancer
and found a significant decrease in the serum beta-carotene levels in male
cases compared to those of the control group. In the present paper, we
will introduce a finding which revealed the possibility that a low serum
carotenoid level may be involved in the development of oral precancer.
Many epidemiological and other studies have shown that the development of oral and other cancers is associated with an insufficient intake of fruits and green and yellow vegetables and that such a risk may decrease with an increased level of micronutrients, namely retinol, beta-carotene, and vitamin E, in the serum. Zheng et al. have reported that a high level of carotenoids such as beta-carotene in the serum is strongly associated with a decreased risk of developing oral cancer. In addition, retinoids (eg. retinol) and carotenoids (eg. beta-carotene) have been conventionally used to treat oral precancer. Oral leukoplakia, a type of keratosis which develops on the oral mucous membrane, is a significant disease regarded as precancer because up to 51.5% of cases may develop into cancer. However, there have been no epidemiological studies which compare the levels of anti-oxidative nutrients in the serum of oral leukoplakia cases to those of healthy people. We thus planned an epidemiological study, which is a case-control study on local inhabitants, in order to clarify the relationship between oral leukoplakia and the levels of these micronutrients in the serum.
Subjects and Methods
During the three years from 1995 through 1998, we conducted medical
checkups for oral cancer on examinees aged 40 or older of general medical
checkups in city T in Aichi Prefecture. The cases were 48 subjects (38
males, aged 62.4±10.0; 10 females, aged 62.1±10.7) who were found at
the checkups to have oral leukoplakia and later tested positive at a confirmatory
examination. All participants of the checkups filled out a questionnaire
with questions about smoking and alcohol consumption. Blood samples were
collected at the checkups, centrifuged, and the serum samples were stored
at -80℃. Four controls for each case were selected out of the group of
examinees who proved negative at the checkups after matching for gender
and age. The levels of micronutrients, namely retinol, alpha-tocopherol,
and carotenoids including zeaxanthin/lutein, cryptoxanthin, lycopene, alpha-carotene,
and beta-carotene in the serum were measured by HPLC. The results were
statistically analyzed for each gender using the t-test and logistic regression
analysis. Data on smoking and alcohol consumption from samples of each
group at baseline were examined using the chi-square test.
Results
There was no statistically significant difference in either gender
between the cases and controls in the distribution of smokers and alcohol
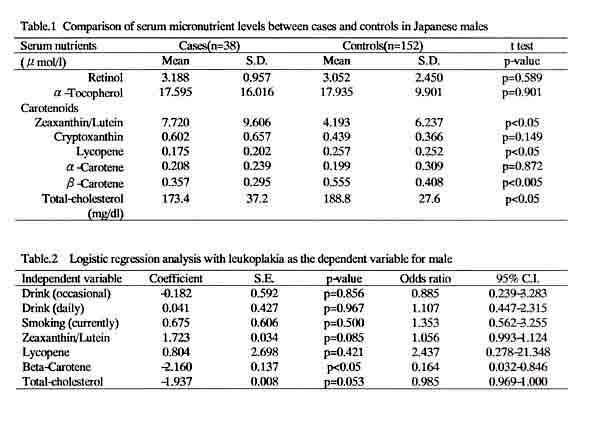
drinkers. The serum micronutrient levels in males are shown in Table 1.
The lower levels of beta-carotene and lycopene shown in leukoplakia cases
were statistically significant (p<0.005 and p<0.05, respectively).
In contrast, higher levels of xeaxhanthin/lutein and cryptoxanthin were
seen in leukoplakia cases, especially the former, which was statistically
significant (p<0.05). There was no significant difference in the levels
of other nutrients. On the other hand, female groups showed no significant
difference between cases and controls in the levels of any of the nutrients.
The results of the logistic regression analysis in which leukoplakia was
a dependent variable and drinking, smoking, and serum carotenoid levels
were independent variables showed that beta-carotene may decrease the risk
of leukoplakia (odds ratio, 0.16; 95% confidence interval, 0.029-0.866)
(Table 2).
Discussion
The results of the present study conducted through an inhabitant-based
epidemiological survey show low levels of beta-carotene and lycopene in
the serum of male oral leukoplakia cases. The multivariate analysis suggests
that a high level of beta-carotene in the serum may decrease the risk of
developing oral leukoplakia. On the other hand, as serum retinol levels
were not shown to be associated with the disease, it is considered that
beta-carotene may decrease the risk without being converted to vitamin
A. These results suggest that beta-carotene may be a more effective chemical
prophylaxis than retinol and alpha-tocopherol, which have conventionally
been clinically used for oral cancer. We are thus planning a clinical intervention
study on the chemoprophylaxis of oral precancer using mainly beta-carotene.
We would like to extend our deepest gratitude to our collaborator Professor
Yoshinori Ito (Fujita Health University).