Report on Committee of investigation for next
revised RDA
"Progress of Dietary Reference Intake"
Sponsor: Japanese Society of Nutrition and Food Science,
Committee of investigation for next revised RDA
(This committee was established by Japanese Society of Nutrition and
Food Science in 2000)
Supporter: ILSI-Japan, Vitamin Information Center (Japan), Meiji Milk
Products Co., Ltd.
Date: May.7 2001, Place: Kyoto International Hall, Japan
Speaker: Dr. Dietrich Hornig , F. Hoffman-La. Roche Ltd
Prof. Naotaka Hashizume, Toho University School of Medicine
Current Trends in the Recommendations
for Vitamin Intake
Dietrich Hornig, Ph.D. F.Hoffmann-LaRoche Ltd
The first RDAs (Recommended Dietary Allowances) were published in 1943
by the National Research Council of the United States with the objective
of "providing standards to serve as a goal for good nutrition in connection
with national defense". Since then, the application of RDAs has broadened
and now serves other purposes, for example in planning and procuring food
supplies, in the interpretation of food consumption data, and as basis
for nutritional labeling values.
Over the recent years, more scientific evidence regarding the role of
vitamins has emerged and expert groups are reviewing these recommendations
in many countries. The US Food and Nutrition Board has established a new
approach in the assessment of requirement. It was mainly influenced by
new scientific results from epidemiological, biochemical, and clinical
studies as well as of studies with vitamins at the molecular level. This
new concept represents a paradigm shift and indicates that nutrient requirement
is no longer determined by avoidance of deficiency (indicated by clinical
manifestation and status), but by its contribution to maximize health and
to increase quality of life (determined by functional parameters including
reduction of risk of chronic disease such as cardiovascular disease, cancer,
eye disease, and osteoporosis). The DRIs (Dietary Reference Intake) values
is to be understood as a collective term for the respective nutrient and
is covering the range from avoidance of deficiency to its potential role
in reducing risk of chronic disease. The new DRIs are the results of an
extensive review of the overall knowledge base, with special emphasis on
human data. DRIs are a set of up to four values: Estimated Average Requirement
EAR, Recommended Dietary Allowance RDA, Estimated Average Intake AI, and
Tolerable Upper Level of Intake UL. Their definitions are as follows:
Estimated Average Requirement (EAR): a daily nutrient intake
value that is estimated to meet the requirement of half the healthy individuals
in a group.
Recommended Dietary Allowance(RDA): the average daily dietary
intake level that is sufficient to meet the nutrient requirement of nearly
all (97 to 98 %) healthy individuals in a particular life stage (age, pregnancy,
lactation) and gender group.
Adequate Intake (AI): a recommended daily intake value based
on observed or experimentally determined approximations of nutrient intake
by a group (or groups) of healthy people that are assumed to be adequate.
The AI is a goal for the nutrient intake of individuals. The AI can be
considered as a surrogate to the RDA if the RDA cannot be determined due
to lack of scientific data.
Tolerable Upper Intake Level(UL): the highest level of daily
nutrient intake that is likely to pose no risk of adverse health effects
to almost all individuals in the general population. As intake increases
above the UL, the risk of adverse effects increases.
Besides the USA, in several other countries new recommendations were
recently published (Germany, Switzerland, Austria (D.A.CH.), France, Japan,
China) and in others the evaluation is either still on-going or is in the
process to be started (e.g. Australia, Netherlands, SEA countries, Nordic
countries). Tolerable Upper Levels of Intake have so far only been assessed
in the USA, Japan and China.
Reports on the most recent evaluations in Germany, Switzerland, Austria
(D.A.CH.), France, Japan, China, Korea and the USA/Canada indicate:
・ An increasing acceptance of the potential role of specific vitamins
in the reduction of risk of chronic diseases, such as the role of vitamins
C and E in cardiovascular disease, the reduction of risk of prostate cancer
with vitamin E, and the role of B-vitamins (folate, vitamins B6 and B12)
in the reduction of risk of cardiovascular disease mediated by homocysteine
・ Increased recommendations for vitamin C: D.A.CH. (100 mg/day );
France (110 mg/day); USA/Canada (75-90 mg/day); Japan (100 mg/day), Korea
(70 mg/day), China (100 mg/day)
・ Additional recommendations for vitamin C in smokers: D.A.CH. (plus
50 mg/day), France (plus 15 mg/day), USA/Canada (plus 35 mg/day
・ An increase in the RDA for Vitamin E: USA/Canada (15 mg alpha-tocopherol/day);
D.A.CH. (15 mg alpha-tocopherol equivalents/day); China (14 mg alpha-tocopherol
equivalents/day)
・ An increase in the RDA for folate: D.A.CH. and USA/Canada (to 400
mg folate/day); Korea (new 250 mg folate/day); China (new 400 mg folate/day)
・ An increase in the recommendation for vitamin K (to 120/90 mg/day);
China (new: 120 mg/day); Japan (new 65/55 mg/day)
・ The recommendation for vitamin A was slightly reduced (USA/Canada:
to 900/700 mg/day). Retinol activity equivalents were introduced with 12
mg of dietary beta-carotene from food sources to be equivalent to 1 mg
retinol activity, or with 2 mg of beta-carotene in oil (supplemental beta-carotene)
to be equivalent to 1 mg of retinol activity. Dietary provitamin A carotenoids
other than beta-carotene (a-carotene; b-cryptoxanthin) require 24 mg to
be equivalent to 1mg of retinol activity.
・ Recommendation to cover part of the requirement as supplements (USA/Canada;
D.A.CH.):
- vitamin B12 in the elderly (USA/Canada: preferentially to be taken
with fortified food or supplements; D.A.CH.: elderly with atrophic gastritis
100 mg/day as supplement)
- additional folic acid as supplement (400 mg folic acid/day) to reduce
the risk of neural tube defects in women of the childbearing age planning
a pregnancy
・ USA/Canada, Japan, and China have introduced tolerable upper levels
of intake (UL) indicating total intake of a vitamin with food, fortified
food, and food supplements which on long term intake does not cause any
adverse effects. D.A.CH. and Korea did not determine tolerable upper levels
of intake, but commented on the safety of vitamins in the text.
・ Japan and China have for the first time issued recommendations for
all vitamins
The various RDA Committees have also elaborated on, which additional
research would be required in order to be able to minimize the current
gaps of knowledge and allowing a satisfactory assessment of the recommendations
and the tolerable upper levels of intake of nutrients. Major research areas
were identified:
・ Studies to estimate average requirement in apparently healthy humans
・ Studies on the nutrient needs of infants, children, adolescents,
pregnant or lactating women
・ Studies to accumulate more evidence on the role of nutrients in
lowering the risk of certain chronic diseases including the validation
of biomarkers
・ Studies on the bioavailability of selected nutrients
Government authorities are now considering the incorporation of these
new science-based recommendations into the legislatory framework by re-assessing
the currently valid so-called labeling RDAs, that are the basis for the
declaration of the vitamin content in fortified foods and food supplements.
Within the European Commission's Scientific Committee on Food and the UK
Ministry of Agriculture, Fisheries and Food, special expert working groups
are currently evaluating the safety of vitamins and minerals. The final
reports are expected to be published by end of this year containing respective
Upper Tolerable Levels of Intake (UL) as basis for the legislation on food
supplements and food fortification, and for labeling the nutrient content
of these products.
Basic Idea and Problems
in the Sixth Revision of the Japanese Recommended
Dietary Allowance
Prof. Naotaka Hashizume, Toho University School of Medicine
Introduction
Recommended Dietary Allowance (RDA) is utilized in many situations
including nutritional guidance and school lunch planning and is the basis
for national health promotion and nutritional policies. It is an index
for the promotion of people's health and the improvement of nutritional
conditions, and many countries in the world have established their own
RDA.
The Japanese RDA is reviewed and revised about every five years based
on the following: changes in living conditions such as food supply and
lifestyles; physical and medical conditions; and improvements in sciences
such as medicine and nutritional science. Recently, the Ministry of Health
and Welfare issued the Sixth Revision of the Japanese Recommended Dietary
Allowance on June 23, 1999. (See 'The Sixth Revision of the Japanese Recommended
Dietary Allowance - Dietary Reference Intakes', Daiichi-Shuppan, 1999.)
Basic Idea
The recent revision introduced a new concept, the "Dietary Reference
Intakes", based on international trends. The Dietary Reference Intakes
show standards for the intake of energy and nutrients for healthy people
for the maintenance and promotion of health and the prevention of lifestyle-related
disease.
Problems
The Japanese Society of Nutrition and Food Science has established
the Dietary Reference Intakes Committee, and its subcommittee chairmen
have given their proposals on the problems in the Sixth Revision of the
Japanese Nutritional Requirements. The following are the vitamin-related
problems which remain to be examined in the future:
1) Isn't the Tolerable Upper Intake Level (UL) for vitamin A too low?
1) While the vitamin D allowance for a Japanese adult is 2.5 ?g, that
for a U.S. adult is 5 ?g, taking into consideration the prevention of osteoporosis.
Isn't the Japanese allowance too small?
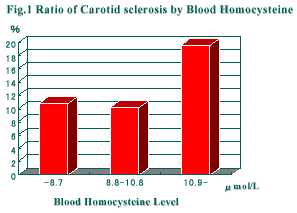
3) The folic acid allowance for a Japanese adult is 200 ?g, while that
for a U.S. adult is 400 ?g. The reason for the U.S. allowance is that keeping
down the levels of homocysteine in the blood, which is a risk factor for
arteriosclerosis, requires 400 ?g of folic acid. The low Japanese allowance
has been criticized by the U.S. and Germany.
4) The U.S. RDA of vitamin C reported in May of 2000 says the allowance
for a male adult is 90 mg and that for a female adult is 75 mg, and the
UL is 2000 mg. The Japanese version says 100 mg regardless of sex and there
is no UL. The Japanese RDA is calculated from Estimated Average Requirements,
which is not used in the calculation of the U.S. version. International
discussion is necessary.
5) Nutrients in breast milk are calculated based on 750 mg in the Sixth
Revision, while that in the Fifth Revision was calculated based on 850
mg. Isn't it necessary for Japan to re-examine the vitamin contents in
breast milk?
Reference) Supplement Advisor system
Our dietary habits have much influence on the recent prevalence of
lifestyle-related disease. Therefore, many people are looking for foods
effective in health maintenance and disease prevention. However, the information
on so-called health foods conveyed every day by mass media including television,
newspaper and magazines does not include sufficient basic information on
the effects of the foods, such as their scientific foundation, generality,
safety and relationship with medical drugs. Under current circumstances,
consumers cannot help being confused by individual pieces of information.
In addition, supplements are considered "medical foods" which are between
foods and medicines. Therefore, they are effective but side effects cannot
be overlooked. It thus became necessary to establish an organization to
provide information on supplements and a system to provide qualified specialists.
Both food manufacturers and pharmaceutical companies are involved in
supplements. Therefore, the Japanese Association of Clinical Nutrition,
which is a non-profit organization, was put in charge of establishing the
Japanese Supplement Advisor Accreditation System.
1. Objective and Roles
The purpose of the supplement advisor system is to educate consumers.
Supplement advisors are merely one component for this plan but are indispensable
for the future education of the general public. Consumers must be responsible
for their own use of supplements, but with today's scattered information
it is difficult to make a correct decision. The role of supplement advisors
is thus to help consumers with making a fair, correct decision. Supplement
advisors must therefore acquire knowledge and technique to make fair, correct
decisions for themselves.
2. Educational Program for Supplement Advisors
Although there will be some difference between centers, the program
will be categorized by required subjects including knowledge on clinical
nutrition, food safety, information and laws and regulations on supplements,
and optional subjects on basic knowledge.
3. Keys to Accreditation
An examination system is necessary in order to insure the quality of
supplement advisors. The examination must be fair and hold good for the
rest of the world as well. In addition, in order to keep up with the progress
of science even after passing the exam, a renewal system is also necessary. |